| Student Info |
|
|
|
ANTERIOR INTERCOSTAL COMPRESSION SYNDROME:
Anterior
Intercostal Compression Syndrome (AICS) was first described by
Dr. Deepak Sebastian as a differential screen for
anterior chest and thoracic pain. It is a condition
where the intercostal space is compromised resulting in
anterior chest and thoracic pain. While intercostal
neuralgia exists as a clinical entity, several other
structures within the intercostal space are speculated
to be potential pain mediators. In the presence of AICS
the exact structures however, are difficult to specify.
When visceral mediation has been ruled out and in the
absence of neuralgic radiating pain, AICS may be
considered. Forward head posture with protracted
scapulae can cause cervical, thoracic and shoulder
dysfunction. |
|
 The
consequence of a forward head posture on the ribs, is
worth mentioning. The upper ribs assist respiration by
moving in a pump handle fashion assisted by the
pectoralis minor which narrows the intercostal space.
Rib widening or the bucket handle movement is assisted
by the serratus anterior which helps widen the
intercostal space (Brand, 2008). This is accomplished
with a fixed scapula whilst stabilizing the ribs from an
excessively anterior displacement (Flynn, 1996).
Dysfunctional states as in a prolonged forward head and
scapula protraction, can render the pectoralis minor
tight and the serratus anterior weak in addition to
other factors (subcranial, cervical and thoracic
dysfunction). This can cause a relative approximation of
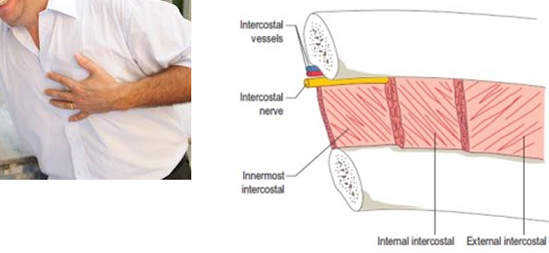
the intercostal space resulting in pain. In the absence
of intercostal neuralgia, the structures within the
intercostal space that are speculated to cause pain are
the periosteum of the ribs, intercostal muscles, and the
intercostal artery and vein. The
consequence of a forward head posture on the ribs, is
worth mentioning. The upper ribs assist respiration by
moving in a pump handle fashion assisted by the
pectoralis minor which narrows the intercostal space.
Rib widening or the bucket handle movement is assisted
by the serratus anterior which helps widen the
intercostal space (Brand, 2008). This is accomplished
with a fixed scapula whilst stabilizing the ribs from an
excessively anterior displacement (Flynn, 1996).
Dysfunctional states as in a prolonged forward head and
scapula protraction, can render the pectoralis minor
tight and the serratus anterior weak in addition to
other factors (subcranial, cervical and thoracic
dysfunction). This can cause a relative approximation of
the intercostal space resulting in pain. In the absence
of intercostal neuralgia, the structures within the
intercostal space that are speculated to cause pain are
the periosteum of the ribs, intercostal muscles, and the
intercostal artery and vein. |
|
Management should hence address all components of a
forward head but more specifically pectoralis minor
stretching, mobilizing the intercostal space into
opening and serratus anterior strengthening.
Differentials include intercostal muscle cramp or tear,
rib fractures, costochondritis, Tietze syndrome, rib
infection or metastasis in rare cases, and
post-operative thoracic surgery, particularly coronary
artery bypass. |
|
References:
Brand, R. A. (2008). "Origin and Comparative Anatomy of
the Pectoral Limb". Clinical Orthopaedics and Related
Research 466 (3): 531.
Flynn TW. ed. The Thoracic Spine and Chest Wall. Boston,
MA: Butterworth-Heinemann; 1996.
Sebastian D. Anterior Intercostal Compression Syndrome.
(In differential screening of regional pain in
musculoskeletal practice 2015; Jaypee Bros, New Delhi,
London, Philadelphia, Panama. |
|
|
THE CERVICAL EXTENSOR ENDURANCE TEST (CEET):
 The
CEET was first described by Dr. Deepak Sebastian as a screen
exam to identify the presence of weakness of the neck
extensors and differentiate the presence of weakness of
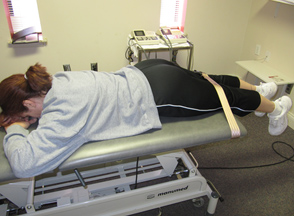
the superficial versus the deep neck extensors. With the
patient lying prone and head and neck past the edge of
the table and the cervico-thoracic junction stabilized,
the ability of the individual to sustain a chin tuck
position in neutral for 20 seconds is evaluated (fig.
a). A positive finding for weakness of the deep neck
extensors is the ‘chin length’ increasing with neck
extension, as observed on the inclinometer, indicating a
dominance of the superficial extensors of the neck (fig.
b). Weakness of both deep and superficial neck extensors
is identified by the presence of neck flexion indicating
an inability to hold the head up (fig. c). 30
individuals with neck pain were examined by 2 raters for
reproducibility, with the study yielding ‘good’ inter-rater
reliability, (k=0.800, SE of kappa = 0.109, 95% CI). The
CEET was first described by Dr. Deepak Sebastian as a screen
exam to identify the presence of weakness of the neck
extensors and differentiate the presence of weakness of
the superficial versus the deep neck extensors. With the
patient lying prone and head and neck past the edge of
the table and the cervico-thoracic junction stabilized,
the ability of the individual to sustain a chin tuck
position in neutral for 20 seconds is evaluated (fig.
a). A positive finding for weakness of the deep neck
extensors is the ‘chin length’ increasing with neck
extension, as observed on the inclinometer, indicating a
dominance of the superficial extensors of the neck (fig.
b). Weakness of both deep and superficial neck extensors
is identified by the presence of neck flexion indicating
an inability to hold the head up (fig. c). 30
individuals with neck pain were examined by 2 raters for
reproducibility, with the study yielding ‘good’ inter-rater
reliability, (k=0.800, SE of kappa = 0.109, 95% CI). |
|
References:
Sebastian D, et, al. The cervical extensor endurance
test: A reliability study. J Bodyw Mov Ther. 2015
Apr;19(2):213-6 |
|
| THE SITTING ACTIVE AND PRONE PASSIVE LAG TEST (SAPLT): |
 |
|
 |
|
|
TEST
POSITION FOR ‘ACTIVE LAG’ |
|
TEST
POSITION FOR ‘PASSIVE LAG’ |
|
|
|
The sitting active and prone passive lag test (SAPLT)
was first described by Dr. Deepak Sebastian to identify the
presence of an active or a passive terminal extension
lag at the knee joint. The lack of terminal extension
and its consequences in the knee have been previously
described. The terms flexion deformity or contracture
have been used and their occurrence has been mostly
associated with post-operative knee surgery,
neurological sequelae and osteoarthritis. Additional
causes described are arthrogenic muscle inhibition (AMI)
secondary to trauma to the knee, inadequate cortical
representation, tightness of the posterior knee capsule,
tightness of the gastrocnemius, popliteus and hamstrings
and injury to the knee extensor mechanism. Terminal
extension in the knee is a pre-requisite for adequate
stability and load distribution during the stance phase
of gait and weight bearing function. The lack of full
extension at the knee can result in a greater force of
quadriceps contraction and energy expenditure. It can
also result in slower walking velocity, abnormal gait
mechanics, overloading the ipsilateral patello-femoral
joint and the contra-lateral limb, resulting in pain and
dysfunction. This includes, but not limited to patello-femoral
pain, gait abnormalities, lower extremity muscle
imbalances, leg length discrepancy and back pain.
Residual flexion contractures after have been associated
with poorer functional scores and outcomes. While some
flexion contractures are obvious others can be subtle
and missed. Additionally it may ‘not’ be a contracture
but a diminished efficiency of the knee extensor
mechanism. The may still result in a lack or lag of
terminal knee extension, with instability and
consequences therein. This simply means that a lack in
terminal knee extension may be secondary to an active or
a passive restraint. Although the prevalence has not
been studied, in clinical practice we observed the
presence of a knee extension lag in most patients with a
knee dysfunction. Since the presence and consequences of
a lack in terminal knee extension is obvious, a reliable
test to appropriately identify its presence led to the
description of the APLT. Additionally, the test was able
to differentiate an active versus as passive restraint,
suggesting the type of intervention needed.
Methods: 56 patients with a diagnosis of knee pain were
randomly assigned and independently examined by two
physical therapists at a time, to determine the presence
of an active or a passive extension lag at the knee. An
active lag was determined by the inability of the
erectly seated subject to actively extend the involved
knee in maximally dorsiflexion of the ankle to the same
level as the normal knee held in maximal extension and
ankle in maximal dorsiflexion, as seen by the levels of
the toes. A passive lag was determined by placing the
subject prone with the knees just past the edge of the
table and determining the high position of the heel in a
fully resting extension position compared to the heel on
the normal side. Results: For the sitting active lag
test, the inter-rater reliability was ‘good’ (Kappa
0.792, SE of kappa 0.115, 95% confidence interval). For
the prone passive lag test, the inter-rater reliability
was ‘good’ (Kappa 0.636, SE of kappa 0.136, 95%
confidence interval). Conclusion: The SAPLT may be
incorporated as a simple yet effective test to determine
the presence of a knee extension lag. It identifies the
type of restraint, active, passive or both, and is
suggestive of the most appropriate management.
|
|
References:
Sebastian D, et al. The sitting active and prone
passive lag test: An inter rater reliability study. J
Bodyw Mov Ther. 2014 Apr;18(2):204-9. |
|
|
T2 RADICULOPATHY:
T2 radiculopathy was first described by Dr. Deepak Sebastian
as a differential screen for radicular pain in the upper
extremity. It is a condition where the second thoracic
nerve is entrapped in the intervertebral foramen between
T2T3 resulting in upper extremity radicular pain.
 The
anterior divisions of the thoracic spinal nerves from T1
to T11 are the intercostal nerves. They exit from the
thoracic spinal column beneath their corresponding
vertebra ( O Connor RC, 2002 ). Each nerve is connected
with the adjoining ganglion of the sympathetic trunk by
a gray and a white ramus communicans. The intercostal
nerves are distributed chiefly to the thoracic pleura
and abdominal peritoneum and differ from the anterior
divisions of the other spinal nerves in that each
pursues an independent course without plexus formation.
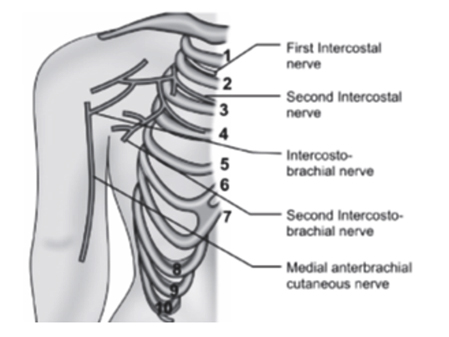
Lateral cutaneous branches are derived from the
intercostal nerves, about midway between the vertebræ
and sternum; they pierce the Intercostales externi and
Serratus anterior, and divide into anterior and
posterior branches. The lateral cutaneous branch of the
second intercostal nerve which exits between T2T3, does
not divide like the other thoracic nerves, into an
anterior and a posterior branch; but midway anterior to
the axilla, gives off a branch, the intercostobrachial
nerve (ICBN. It pierces the intercostalis externus, the
serratus anterior, crosses the axilla to the medial side
of the arm, and joins with a filament from the medial
brachial cutaneous nerve. It then pierces the fascia,
and supplies the skin of the upper half of the medial
and posterior part of the arm, communicating with the
posterior brachial cutaneous branch of the radial nerve
which supplies the lateral forearm (Loukas M 2006). A
second intercostobrachial nerve is frequently given off
from the lateral cutaneous branch of the third
intercostal which supplies filaments to the axilla and
medial side of the arm (Fig). One can assume that the
ICBN is the communicating link between T2 spinal nerve
and the upper extremity. Thus the sequence of events
resulting in a T2 radiculopathy involve the T2 spinal
nerve, adjoining intercostobrachial nerve, medial
antebrachial cutaneous nerve and the posterior brachial
cutaneous branch of the radial nerve. The
anterior divisions of the thoracic spinal nerves from T1
to T11 are the intercostal nerves. They exit from the
thoracic spinal column beneath their corresponding
vertebra ( O Connor RC, 2002 ). Each nerve is connected
with the adjoining ganglion of the sympathetic trunk by
a gray and a white ramus communicans. The intercostal
nerves are distributed chiefly to the thoracic pleura
and abdominal peritoneum and differ from the anterior
divisions of the other spinal nerves in that each
pursues an independent course without plexus formation.
Lateral cutaneous branches are derived from the
intercostal nerves, about midway between the vertebræ
and sternum; they pierce the Intercostales externi and
Serratus anterior, and divide into anterior and
posterior branches. The lateral cutaneous branch of the
second intercostal nerve which exits between T2T3, does
not divide like the other thoracic nerves, into an
anterior and a posterior branch; but midway anterior to
the axilla, gives off a branch, the intercostobrachial
nerve (ICBN. It pierces the intercostalis externus, the
serratus anterior, crosses the axilla to the medial side
of the arm, and joins with a filament from the medial
brachial cutaneous nerve. It then pierces the fascia,
and supplies the skin of the upper half of the medial
and posterior part of the arm, communicating with the
posterior brachial cutaneous branch of the radial nerve
which supplies the lateral forearm (Loukas M 2006). A
second intercostobrachial nerve is frequently given off
from the lateral cutaneous branch of the third
intercostal which supplies filaments to the axilla and
medial side of the arm (Fig). One can assume that the
ICBN is the communicating link between T2 spinal nerve
and the upper extremity. Thus the sequence of events
resulting in a T2 radiculopathy involve the T2 spinal
nerve, adjoining intercostobrachial nerve, medial
antebrachial cutaneous nerve and the posterior brachial
cutaneous branch of the radial nerve.
The vulnerability of the upper thoracic spine to
mechanical dysfunction is described by various sources
(Arana E 2004). As is the case with the lumbar and
cervical spine, degeneration of the posterior spinal
elements of the thoracic spine is an inherent source of
axial back pain and radiculopathy. (Vanichkachorn JS,
and Vaccaro AR) suggest generators of thoracic radicular
pain to be musculoskeletal, neurological, infectious,
visceral, metabolic and congenital. Among the
musculoskeletal causes, spondylosis, disc disease and
somatic causes have been mentioned. (Edmondston et al)
investigated the influence of whole body sitting posture
on cervico-thoracic posture, mechanical load and
extensor muscle activity in 23 asymptomatic adults. They
concluded that the more neutral sitting postures reduce
the demand on the cervical extensor muscles and modify
the relative contribution of cervical and thoracic
extensors to the control of head and neck posture. They
suggest postures that promote these patterns of muscular
activity may reduce posture related pain suggesting
muscle weakness and imbalances to be contributors of
neck and upper thoracic pain.
Somatic dysfunction in the upper thoracic region may be
postural, or acquired secondary to systemic disorders
e.g. asthma. The key contributor to dysfunction is the
forward head posture, which comprises upper cervical
extension, lower cervical flexion, upper and lower
thoracic kyphosis. This could lead to considerable
hypomobility of the thoracic spine ( Lounardi AC 2011).
The forward head posture is typically associated with
weakness of the deep cervical flexors and the thoracic
extensors ( Watson Trott 1993). The above factors
collectively favor the presence of degenerative and
mechanical dysfunction of the upper thoracic region.
While upper thoracic spine is vulnerable for
degenerative and mechanical dysfunction, the potential
for irritation of the intercostobrachial nerve exists,
if the T1T2, T2T3 segments are involved, resulting in
upper extremity radicular pain. Complaints of upper
thoracic pain with pain radiating into the arm, the
presence of upper thoracic somatic dysfunction,
restricted cervical mobility (especially extension) and
pressure mechanosensitivity over the lateral aspect of
the thoracic vertebrae causing radiating pain into the
arm, may be diagnostic indicators. |
|
References:
Sebastian D. T2 radiculopathy: A differential screen
for upper extremity radicular pain. Physiother Theory
Pract. 2013 Jan;29(1):75-85. |
|
|
TRIANGULAR INTERVAL SYNDROME:
Triangular Interval Syndrome (TIS) was first described by Dr.
Deepak Sebastian as a differential diagnosis for
radicular pain in the upper extremity. It is a condition
where the radial nerve is entrapped in the triangular
interval resulting in upper extremity radicular pain.
The triangular interval is the space that is triangular
in shape, situated between the long head and lateral
head of the triceps brachii and the teres major.
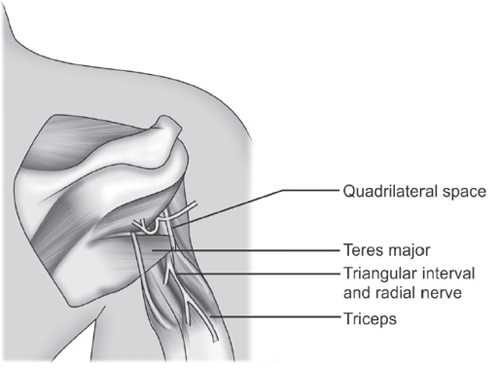 The
radial nerve and profunda brachii pass through the
triangular interval and are hence vulnerable. The
triangular interval has a potential for compromise
secondary alterations in thickness of the teres major
and triceps (McClelland 2007). They described based on
cadaveric studies that fibrous bands were commonly
present between the teres major and triceps. When these
bands were present, rotation of the shoulder caused a
reduction in cross sectional area of the space. Normal
resting postures of humeral adduction and internal
rotation with scapular protraction may be speculated as
a precedent for teres major contractures owing to the
shortened position of this muscle in this position. In
addition, hypertrophy of this muscle can occur secondary
to weight training and potentially compromise the
triangular interval with resultant entrapment of the
radial nerve (ABY Ng et al 2003). The
radial nerve and profunda brachii pass through the
triangular interval and are hence vulnerable. The
triangular interval has a potential for compromise
secondary alterations in thickness of the teres major
and triceps (McClelland 2007). They described based on
cadaveric studies that fibrous bands were commonly
present between the teres major and triceps. When these
bands were present, rotation of the shoulder caused a
reduction in cross sectional area of the space. Normal
resting postures of humeral adduction and internal
rotation with scapular protraction may be speculated as
a precedent for teres major contractures owing to the
shortened position of this muscle in this position. In
addition, hypertrophy of this muscle can occur secondary
to weight training and potentially compromise the
triangular interval with resultant entrapment of the
radial nerve (ABY Ng et al 2003).
Shoulder dysfunctions have a potential for shortening
and hypertrophy of the teres major. Shoulders that
exhibit stiffness, secondary to capsular tightness,
contribute to contracture and hypertrophy of the teres
major (Jiu-jenk Lin 2006). Hence, restricted external
rotation can encourage adaptive shortening and
thickening of the internal rotators of the shoulder
principally the teres major and subscapularis. One may
speculate that the lateral arm pain presented in
shoulder dysfunctions may be of a nerve origin secondary
to adverse neural tension of the radial nerve.
The triceps brachii has a potential to entrap the radial
nerve in the triangular interval secondary to
hypertrophy. The presence of a fibrous arch in the long
head and lateral head further complicates the situation.
Repeated forceful extension seen in weight training and
sport involving punching may be a precedent to this
scenario (Manske 1977, Prochaska 1993, Ng 2003). The
radial nerve is vulnerable as it passes through this
space, for all of the reasons mentioned above. Awareness
of the potential existence of this condition may assist
clinicians in their clinical decision making process.
|
|
References:
Sebastian D. Triangular Interval Sydrome. A
differential diagnosis for upper extremity radicular
pain. Physiother Theory Pract. 2010 Feb;26(2):113-9. |
|
|
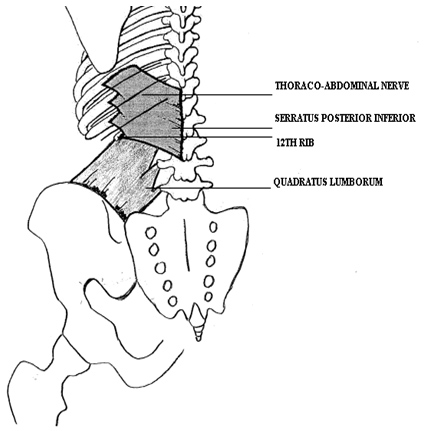
THE LOWER THORACIC SYNDROME
Lower Thoracic Syndrome was first described by Dr. Deepak
Sebastian as a differential screen for back pain
occurring in the lower thoracic region and flank area. A
history of a vertical compression injury as in a fall on
the buttock may favor it’s presence. The lower thoracic
region, unlike the upper and mid thoracic region, is
infrequently described as a source of musculoskeletal
pain and dysfunction. The two clinical entities
described to cause pain in this region are
intervertebral disc herniation and thoracolumbar
junction syndrome. The T11, T12 vertebra has been
described to be vulnerable for injury, the mechanisms
which include vertical compression and flexion
compression. These however are described to cause stable
or unstable fractures of the vertebra. While the
vulnerability of the T11, T12 vertebra for fractures has
been adequately presented, traumatic vertical
compression injuries that do not result in a fracture
are remotely described. The need being obvious secondary
to the common occurrence of slips and falls on the
buttock in slippery conditions. It is suggested that
when bony disruption does not occur in a traumatic
event, the structures of the vertebral motion segment
which includes the facet joint, exiting nerve root and
supporting muscles and ligaments are subjected to
stress, consequently resulting in dysfunction. Thus
several structures in the lower thoracic region,
especially when the mechanism of injury is a vertical
compression, are susceptible. They are, the vertebral
motion segments of the lower thoracic spine, the
thoracoabdominal nerves, the 12th rib, the quadratus
lumborum and the serratus posterior inferior. They are
speculated to be potential symptom mediators and
collectively identified as vulnerable structures in
lower thoracic syndrome.
VULNERABLE STRUCTURES IN NON TRAUMATIC VERTICAL
COMPRESSION
 |
|
References:
Sebastian D. Lower Thoracic Syndrome-a differential
screen for back pain following vertical compression
injury: a case report. J Bodyw Mov Ther. 2014
Oct;18(4):545-52. |
|
|
THE SCAPULA BACKWARD TIPPING TEST (SBTT):
 The
Scapula Backward Tipping Test (SBTT) was first described by
Dr. Deepak Sebastian to identify the presence of forward
tipping of the scapula. Forward tipping of the scapula
has been described to encourage shoulder dysfunction and
a reliable method to identify it’s presence is hence
mandatory. The attributes to this dysfunction are
tightness of the coraco-clavicular ligaments, pectoralis
minor and teres major. The subject is placed prone with
the head and neck supported and palms in the anatomical
position. The examiner places one hand on the inferior
angle of the scapula and the fingers of the other hand
hook under the coracoid process. A gentle pull is
imparted in the upward direction to sense tightness.
Care is taken to not hook the fingers under the clavicle
as this may encourage over stretching of the
acromio-clavicular joint. Comparison is made with the
non-symptomatic side to improve sensitivity of the
testing procedure. This test has been found to be
reproducible between examiners and sensitive to the
symptomatic side, thereby improving it’s diagnostic
utility. The
Scapula Backward Tipping Test (SBTT) was first described by
Dr. Deepak Sebastian to identify the presence of forward
tipping of the scapula. Forward tipping of the scapula
has been described to encourage shoulder dysfunction and
a reliable method to identify it’s presence is hence
mandatory. The attributes to this dysfunction are
tightness of the coraco-clavicular ligaments, pectoralis
minor and teres major. The subject is placed prone with
the head and neck supported and palms in the anatomical
position. The examiner places one hand on the inferior
angle of the scapula and the fingers of the other hand
hook under the coracoid process. A gentle pull is
imparted in the upward direction to sense tightness.
Care is taken to not hook the fingers under the clavicle
as this may encourage over stretching of the
acromio-clavicular joint. Comparison is made with the
non-symptomatic side to improve sensitivity of the
testing procedure. This test has been found to be
reproducible between examiners and sensitive to the
symptomatic side, thereby improving it’s diagnostic
utility.
|
|
References:
Sebastian D, Chovvath R, Malladi R. The scapula backward
tipping test: An inter-rater reliability study. Journal
of Bodywork & Movement Therapies. 2017; 21: 69-73. |
|
__________________________________________________________________________________________________________________________________________________
DEPENDENT HEAD
POSTURE DIZZINESS SYNDROME (DHPDS):
Dependent head
posture dizziness syndrome was first described by Dr. Deepak Sebastian and Dr.
Van Chockalingam. The structural and functional correlation of the semicircular
canals of the inner ear and cervical facets have been described for the first
time. While the importance of segmental cervical mobility in maintaining
ocular- cervical equilibrium has been highlighted, the importance of cervical
mobility and alignment in preventing dislodgement of degenerating otoconia
during dependent head postures is also outlined. The importance of restoring
functional cervical mobility during routine vestibular rehabilitation is
emphasized.
References:
Sebastian D, Chockalingam S, Patel C. Dependent head posture dizziness syndrome: a case report. Int Phy Med Rehab J. 2022; 7(2): 56-65.
|
|